One of the major draw backs to standard, open carpal tunnel release was
the slowness of recovery in the palm side surgical scar. Often, the 2 inch
palm side scar would remain sensitive to direct pressure for approximately
six to eight weeks. in the working patient, this scar sensitivity could
preclude return to normal work activities. Recently, orthopedic technology
has advanced to the point where a standard arthroscope has been specially
modified to be of use in carpal tunnel surgery.
To employ the endoscopic technique in carpal tunnel release, a small
1/2 inch horizontal incision is made at the wrist and the arthroscope is
introduced underneath the transverse carpal ligament. A cannula is
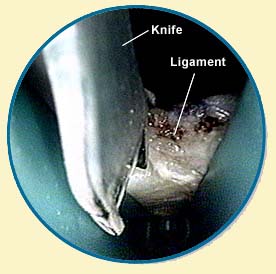
inserted into the hand, just under the offending ligament. The surgeon
looks through a scope and uses a small knife to simply cut the ligament,
thus freeing the nerve. A special blade attached to the tip of the
arthroscope is then utilized to incise the transverse carpal ligament from
the inside of the carpal tunnel. In effect, by cutting through the
transverse carpal ligament, the compression on the median nerve is
alleviated and the nerve is thus allowed to go on the heal. With nerve
healing, the painful wrist syndrome is corrected.
Endoscopic carpal tunnel surgery is performed on an outpatient basis
utilizing a local anesthetic to numb the arm. After the procedure, a
splint is applied to the wrist and the patient is discharged and allowed
to go home. Within a week, the splint is removed, a temporary wrist splint
is applied and hand rehabilitation is initiated.